
No One Plans for the Neonatal Intensive Care Unit (NICU)
No one plans to need the NICU.
Sometimes you’ve been told for weeks that it might happen. Sometimes it’s a total surprise. Either way, walking into the NICU can feel overwhelming, clinical, and disorienting—especially when you’re still recovering from birth.
This post is here to gently orient you. To help you know what you might see, what you can ask for, and when it’s time to call in extra support—for you and your baby.
You don’t need to memorize this. Just know you’re allowed to take up space, ask questions, and receive care too.
What It’s Like to Walk Into the NICU
The NICU is often bright, busy, and full of sounds—monitors beeping, alarms chiming, staff moving quickly. Babies may be in isolettes (incubators) or open cribs, oftentimes with wires and tubes that makes everything feel so scary and overwhelming.
It can be shocking to see your baby like this, even if you knew it was coming.
A few things to know:
Monitors can look scarier than they are. Many alarms are set very conservatively and can go off with normal baby movements.
NICU nurses are highly specialized. They often care for just one or two babies at a time and get to know them deeply. You might hear a nurse refer to your newborn as “my baby.” Don’t take it personally — it’s not literal. It just reflects their dedication and the emotional investment they have in the babies they care for.
Baseline equipment: Most NICU babies have a pulse oximeter and telemetry wires (to track heart rate and breathing). Your baby may have more or fewer attachments depending on their age, condition, and length of stay.
Daily rounds: A team of professionals — doctors, nurses, respiratory therapists, dietitians, and sometimes PT, OT, or SLP — discusses your baby’s care. These discussions often happen at the bedside so you can be included.
You are not a visitor. You are your baby’s parent.
If anyone makes you feel otherwise, talk to me. :)
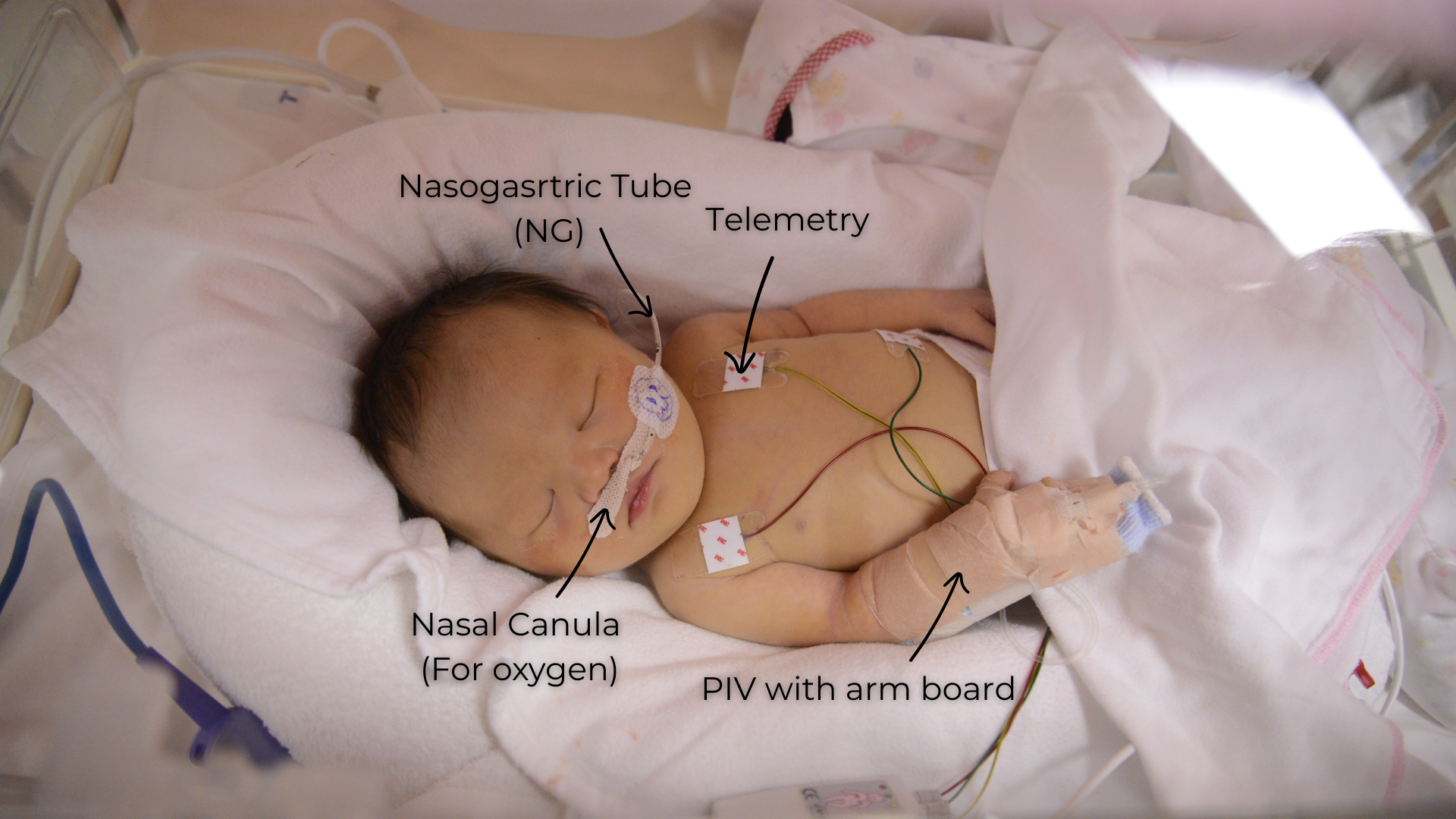
The Equipment (with photos!)
Like I said before, almost every baby who spends time in the NICU — even babies who are there “just for observation” — will have a few pieces of standard equipment attached.
Telemetry or EEG leads are small stickers and wires placed on baby’s chest. These track heart rate and respiratory (breathing) rate so the medical team can continuously monitor how baby is doing without disturbing them.
A pulse oximeter (often wrapped around a hand or foot) measures how much oxygen is in your baby’s blood. It gives real-time feedback about how well baby is oxygenating.
Temperature Monitoring
Most babies born before 34 weeks will also start out with a temperature probe on their body. This allows nurses to continuously monitor baby’s temperature without needing to wake or handle them every three hours to take vitals. Less handling = more rest, which is a big deal for these tiny nervous systems.

Oxygen Support
Some babies need a little extra help with breathing and will have what’s called a nasal cannula. This is a small, soft tube that sits just inside the nostrils and delivers additional oxygen.
The goal here isn’t to replace breathing — it’s to make breathing easier, so baby doesn’t have to work as hard or burn extra energy just to get oxygen.
Feeding Tubes (NG & OG Tubes)
Babies born at 35 weeks and earlier will also typically have a feeding tube. You’ll most often hear this called an NG tube (nasogastric tube).
An NG tube goes through the nose and into the stomach and is how many NICU babies get their nutrition early on. Feeding this way helps conserve energy — babies don’t have to burn precious calories learning to coordinate sucking, swallowing, and breathing before they’re developmentally ready.
Some babies will instead have an OG tube (orogastric tube). This tube goes through the mouth rather than the nose.
OG tubes are commonly used when a baby already has equipment on their nose — like a nasal cannula, CPAP, or other respiratory support — and there simply isn’t space for a tube to also pass through the nostrils comfortably.
Functionally, NG and OG tubes do the same job: they get milk into baby’s stomach safely and efficiently while protecting energy for growth and healing.
Eating is work for babies, and in the NICU, we’re always asking: What can we do to help baby grow without asking their body to do too much, too soon?

IV Access (PIV)
Some babies will also have a PIV, which stands for peripheral intravenous line.
A PIV is a small IV placed in a hand, foot, arm, or leg.
The PIV It allows the medical team to give fluids, nutrition, sugar (glucose), or medications directly into baby’s bloodstream when needed.
This is something I watched very closely as a physical therapist in the NICU, because long periods of arm extension aren’t ideal for a baby’s development. That said, the IV is the priority, so this support is important while it’s in place.
Once the IV comes out, we focus on lots of positive touch, movement, and flexion opportunities to help baby’s body find balance again.
A PIV is temporary — often used early on while feedings are being established or while baby needs a little extra support. These IVs are closely monitored and removed as soon as baby no longer needs them.
IV Access (PIV)
Some babies will also have a PIV, which stands for peripheral intravenous line.
A PIV is a small IV placed in a hand, foot, arm, or leg.
The PIV It allows the medical team to give fluids, nutrition, sugar (glucose), or medications directly into baby’s bloodstream when needed.
This is something I watched very closely as a physical therapist in the NICU, because long periods of arm extension aren’t ideal for a baby’s development. That said, the IV is the priority, so this support is important while it’s in place.
Once the IV comes out, we focus on lots of positive touch, movement, and flexion opportunities to help baby’s body find balance again.
A PIV is temporary — often used early on while feedings are being established or while baby needs a little extra support. These IVs are closely monitored and removed as soon as baby no longer needs them.
Your Role: You Are Part of the Care Team
Even in a highly medicalized space, your presence matters.
Things that only you can do:
• Learn your baby’s cues
• Offer your voice, smell, and touch
• Advocate for comfort, feeding, and bonding
• Notice subtle changes others might miss
You don’t need medical language to be taken seriously. You just need to speak.
What to Advocate For (Even If It Feels Hard)
1. Skin-to-Skin (Kangaroo Care)
If your baby is stable, ask:
• “When can we do skin-to-skin?”
• “What needs to happen to make that possible today?”
Skin-to-skin helps with:
• Temperature regulation
• Breathing and heart rate stability
• Milk supply
• Nervous system regulation (for both of you)
Even very small or medically fragile babies often can do skin-to-skin with planning and support.
2. Feeding Support Early and Often
Whether your baby is:
• Breastfeeding
• Bottle-feeding
• Tube-fed
• Or not feeding yet
You can ask for:
• An IBCLC with NICU experience
• A Speech and Language Pathologist who specializes in infant feeding and swallowing.
Support with pumping that protects your supply
• A feeding plan that looks ahead, not just at today
I have worked with families whose baby was born at 30 weeks, spent 11 weeks in the NICU, and only bottle fed starting at 36 weeks… but after she went home, ended up exclusively breastfeeding. It IS possible, and there are experts out there (us!) who can help.
If feeding feels confusing, emotional, or stressful—that’s a sign to ask for help, not a sign you’re failing.
3. Developmentally Supportive Care
NICU care is about survival and long-term development.
You can ask about:
• If your baby is born before 32 weeks, ask about cycled lighting and how they plan to protect your baby’s sensory development including vision, hearing, and touch.
Positioning and containment (instead of babies lying flat- they should always be flexed as if they were still in the womb to help develop their bone density!)
• Minimizing unnecessary handling (your baby(ies) need sleep to heal their brains and to grow!)
• Clustered care to protect sleep (Ask: What are my baby’s care times? So that you know exactly what time you should be there- usually I tried to arrive about 10 min before the care time for my physical therapy intervention and to help train families, but always ask your nurse!)
• When OT/PT/SLP might be involved
These supports matter for the nervous system and future feeding, movement, and regulation. Every baby in the NICU could benefit from a visit from a PT or OT or SLP trained to support you- if it doesn’t happen in the NICU, ask us how we can help! You can always text us at 971-351-2714.
4. Clear Communication
It’s okay to say:
• “Can you explain that in a different way?”
• “What are we watching for right now?”
• “What would make you more concerned?”
If something doesn’t make sense, pause the conversation. You deserve clarity.
When to Ask for Extra Support
Ask for emotional support if:
• You feel numb, panicky, or detached
• You’re avoiding the NICU or feel frozen when you’re there
• You’re blaming yourself
• You can’t sleep or eat even when you have the chance
Many NICUs have:
Developmental care teams (PT, OT, Speech, IBCLCs, specially trained RNs)
Social workers
Psychologists
Parent support programs
These are not “last resort” resources. They are preventative care.
Ask for feeding or body-based support if:
• You plan to exclusively breastfeed
Your baby is born before 39 weeks and feeding feels stressful or pressured
• Your baby arches, coughs, shuts down (falls asleep or closes their eyes), or seems uncomfortable during feeds
• You’ve been told “they’ll grow out of it” but your gut says otherwise
Early support can change the trajectory—for feeding, bonding, and recovery at home. There are “infant feeding specialists” in many units who are Speech and Language Pathologists and Occupational Therapists (this is who we have on our team at Be Well Baby!) who have special tra
Ask for discharge planning support early
You don’t have to wait until the last 48 hours.
Ask:
• “What should we be working toward before discharge?”
• “What resources can you point us towards for our baby’s development?” (That’s where The Beyond Birth Blueprint comes in!)
“What support will we need at home?”
• “Who do we follow up with after we leave?”
NICU discharge is a transition, not an ending. You deserve continuity of care.
A Note for Parents Who Are Trying to Be “Strong”
You don’t get bonus points for doing this alone.
The NICU is intense because it asks parents to:
• Love deeply
• Wait constantly
• Hand over control
• Make decisions while exhausted and healing
That is a lot.
Support is not a luxury. It’s part of good care.
You and Your Baby Are More Than a Diagnosis
The NICU focuses on numbers, milestones, and timelines—but your baby is a whole person. And so are you.
There is room here for:
• Gentleness
• Questions
• Advocacy
• Connection
And there is life after the NICU—one that often benefits from thoughtful, nervous-system–informed support.
If you’re navigating NICU life now or recovering from it later, you don’t have to do it alone.
Love,
Emily