
Charlie Horses vs. Blood Clots
It's 3am. You're finally asleep — deeply, blissfully asleep — and then your calf seizes up like it's trying to turn itself inside out and you're wide awake, gasping, trying to remember if you're supposed to point your toes or flex them.
Welcome to pregnancy. That was a Charlie horse, and if you've had one, you know exactly what I'm talking about.
Most of the time, that 3am calf cramp is exactly what it feels like — a muscle cramp, nothing more. But during pregnancy and the postpartum period, there's something else I need you to know about: deep vein thrombosis (DVT), or a blood clot in the leg.
These two things can feel similar enough to cause confusion, and that confusion can go in one of two directions — either unnecessary panic over a normal Charlie horse, or (the one that worries me more) dismissing real DVT symptoms because "it's probably just a cramp."
So let's talk about both. You deserve to know the difference.
First, the Charlie Horse
Leg cramps during pregnancy are incredibly common, especially in the second and third trimesters. We're talking up to half of all pregnant people experience them — so if you're waking up in the night with your calf in a vice grip, you are not alone and you are not doing anything wrong.
Here's what's going on: your blood volume has expanded significantly, your uterus is putting pressure on the vessels and nerves that run down your legs, your body's mineral balance is shifting, and you're probably not moving around as freely as you used to. Add in some dehydration and a long day on your feet (or not enough time on your feet), and a Charlie horse is pretty much your body saying it's had enough.
Common contributors include:
Magnesium and calcium shifts during pregnancy
Increased pressure on nerves and blood vessels from a growing uterus
Dehydration
Prolonged sitting or standing without movement breaks
Poor circulation, especially later in pregnancy
The hallmark of a Charlie horse: it comes on suddenly, it's intense, and it resolves within a few minutes — especially if you flex your foot (toes up toward your shin, not pointed). It may leave your calf feeling sore the next day, but the acute cramp passes.
What helps: staying hydrated, daily movement, stretching your calves before bed, and talking to your provider about magnesium supplementation if cramps are frequent.
Now, DVT — and Why Pregnancy Matters Here
A deep vein thrombosis is a blood clot that forms in a deep vein, most commonly in the lower leg, thigh, or pelvis. And here's what I want you to really understand: pregnancy and the postpartum period are some of the highest-risk times in a person's life for developing one.
That's not meant to be alarming — it's meant to be informative. Here's the physiology:
During pregnancy, your blood naturally becomes more prone to clotting. This is a protective mechanism — your body is preparing for the blood loss that comes with delivery. But that same hypercoagulability means clots can form more easily in places we don't want them. Layer on top of that the fact that your growing uterus slows the return of blood from your legs, and you have what's called Virchow's Triad: hypercoagulability, slowed blood flow, and vascular changes. That's the trifecta that makes clots more likely.
The postpartum period — especially those first 6 weeks — actually carries some of the highest DVT risk of all.
Additional risk factors that increase your chances:
Personal or family history of DVT or clotting disorders
C-section delivery
Prolonged bed rest or limited mobility
Long-distance travel (even a 4-hour car ride counts)
Dehydration
Obesity
Multiple gestation (twins, triplets)
Varicose veins
If several of these apply to you, that's worth a conversation with your OB or midwife — not a reason to panic, but a reason to be proactive.
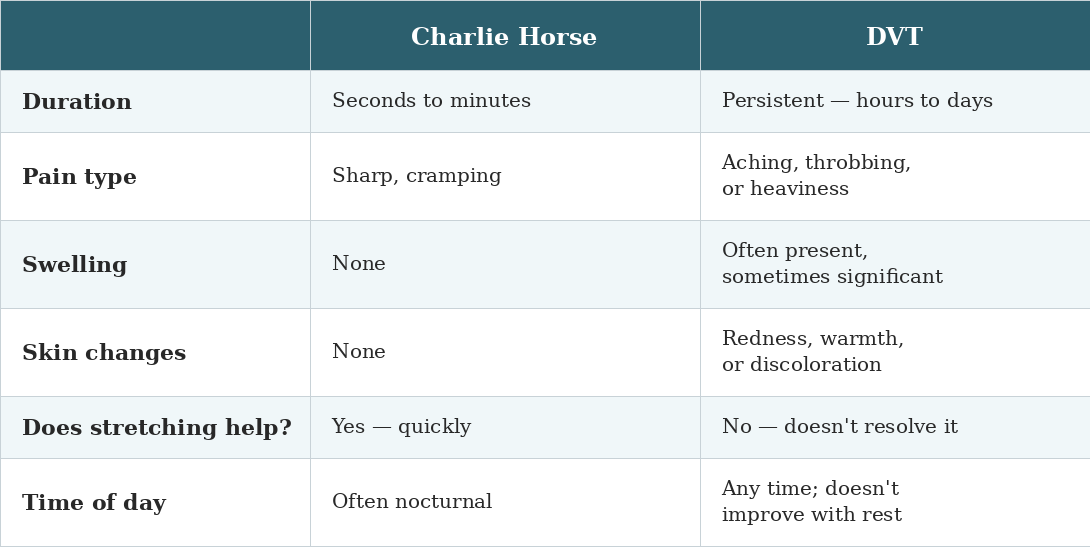
So How Do You Tell the Difference?
This is the question I get asked most often, and I want to give you a real answer.
The honest truth is: sometimes in the moment, it's genuinely hard to know for certain. But there are clear distinguishing features, and I want you to know them.
© 2026 Dr. Emily Spaeth, LLC
The three things that most concern me and should prompt you to call your provider:
One leg is noticeably more swollen than the other
The pain or discomfort doesn't go away — it persists for hours
The area is warm, red, or the skin looks discolored
When to Stop Reading This and Get Help
If you're experiencing any of the following, please don't finish this blog post. Call your provider or go to urgent care or the ER:
Leg pain that doesn't resolve after several minutes
One leg is visibly swollen, especially asymmetrically
Redness, warmth, or skin changes on the calf or thigh
Sudden shortness of breath, chest pain, rapid heart rate, or dizziness — call 911, as these may indicate a pulmonary embolism
I want to be really clear about this: a DVT that goes untreated can break free and travel to the lungs, becoming a pulmonary embolism, which is life-threatening. When it comes to these symptoms, there is no "wait and see."
A Note on Clotting Disorders
Some people have an underlying thrombophilia — an inherited or acquired condition that makes their blood more prone to clotting than average. Examples include Factor V Leiden, Protein C or S deficiency, antithrombin deficiency, and antiphospholipid syndrome.
Many people don't know they have one of these conditions until pregnancy surfaces the risk. If you have a personal or family history of DVT, unexplained recurrent pregnancy loss, stroke at a young age, or a clotting event that seemed out of place — it's worth asking your provider about thrombophilia screening.
Having a clotting disorder doesn't mean pregnancy isn't possible or isn't safe. It means your care team needs the full picture so they can support you appropriately — which might include monitoring, prophylactic blood thinners, or specialist co-management.
What You Can Do to Reduce Your Risk
You can't fully eliminate DVT risk during pregnancy and postpartum, but you can meaningfully lower it:
Move regularly — even 10-minute walks throughout the day make a difference for circulation
Stay hydrated, especially in the third trimester and postpartum
Wear compression stockings if your provider recommends them, especially on travel days
Avoid sitting for long stretches without getting up and moving
After a C-section or any extended hospital stay, prioritize early ambulation (getting up and walking or even just ankle pumps!!) is one of the most protective things you can do
Share your full history and risk factors with your care team — they can't support what they don't know
Most of the time, that 3am cramp really is just a Charlie horse. But you deserve to know the difference, and you deserve care that takes your symptoms seriously — not care that brushes off leg pain as "just pregnancy."
Trust your gut. If something feels off, reach out to your provider. No question about pain, swelling, or discomfort during pregnancy or postpartum is too small.
You are not being dramatic. You are being informed.
Love, Emily
*This post is for educational purposes only and does not constitute medical advice. If you are experiencing symptoms of DVT or pulmonary embolism, please contact your healthcare provider or seek emergency care immediately.
Want more evidence-based support during pregnancy and postpartum? Learn about the Beyond Birth Blueprint or explore more resources at bewellbaby.org/blog.